
ADHD (Attention Deficit Hyperactivity Disorder) is commonly seen as a childhood condition. Yet symptoms persist into adulthood for roughly two-thirds of those affected, with adult prevalence estimated at 2-5%. What happens when these individuals reach old age? And could their genetic predisposition also affect their partners’ health? Our recent study addresses these overlooked questions.
Using data from the English Longitudinal Study of Ageing, which tracks over 7,000 individuals aged 50 and above in England, we examined how genetic predisposition to ADHD relates to health and wellbeing in later life. Rather than relying on clinical diagnoses, which are poorly adapted to older populations, we used polygenic scores, an objective genetic measure that captures the full spectrum of ADHD-related traits.
Our findings are striking. Older adults with higher genetic risk for ADHD experience significantly worse outcomes across multiple dimensions: lower quality of life, greater physical limitations, more mobility difficulties, and higher rates of depression. These associations are not trivial. For instance, a one-standard-deviation increase in genetic ADHD risk corresponds to an 11% increase in functional limitations and a nearly 10% increase in mobility difficulties.
Gender matters considerably. Women show stronger adverse associations, particularly for mobility problems and depression, despite ADHD being historically studied mostly in males. Education, marriage, and higher income provide some protection, suggesting that socioeconomic resources help buffer the impact of genetic risk.
Perhaps our most novel finding concerns spousal spillovers. Husbands’ genetic risk for ADHD significantly harms their wives’ health across all dimensions studied, including quality of life, physical health, depression, and social isolation. Remarkably, the reverse is not true: wives’ genetic risk does not significantly affect husbands’ outcomes (see Figure 1). This asymmetry likely reflects gendered patterns in caregiving and emotional labour within households.
Figure 1: Analysis of Cross-spouse Spillover Effects.
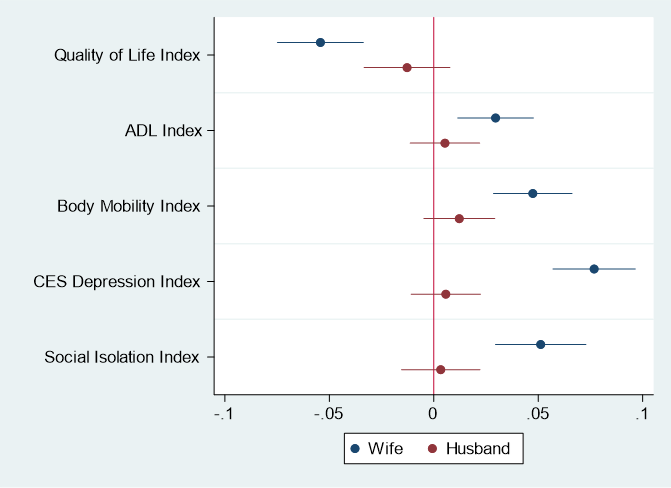
Source: Authors’ own elaboration using data from the English Longitudinal Study of Ageing (ELSA).
These results carry important policy implications. First, ADHD screening and treatment must extend well beyond childhood. Second, health systems should adopt gender-sensitive approaches, recognizing that women bear a double burden from their own genetic risk and their partners’. Third, interventions should target couples rather than individuals alone, since ADHD’s consequences extend to the household level. Finally, reducing socioeconomic inequalities could help mitigate the adverse effects of genetic predisposition.
ADHD is not just a childhood condition. Its consequences reach across the lifespan and beyond the individual, affecting those closest to them.

PhD in Economics, University of Nottingham (UK). Professor in Econometrics, Faculty of Economics and Business Sciences. Expertise in impact evaluation methods applied to public policies, health economics, and education economics.

PhD in Economics, University of Barcelona (ESP). Full Professor in Applied Economics. Expertise in Health Economics and Quantitative Analysis. Extensive research using impact evaluation techniques. Over 1000 citations in Google Academics, H index: 20.

PhD Economics, University of York (UK). Full Professor since 2021. Expertise in evaluation of public policies and Health Economics. Principal investigator in two previous related R+D projects. Over 1000 citations in Google Academics, H index: 16.